SPPB as a Predictor of Adverse Outcomes
Beyond scoring lower-extremity function, SPPB independently predicts mortality, fall risk, and mobility disability in community-dwelling older adults.
The SPPB captures the cumulative burden of age-related functional decline across balance, gait, and lower-limb strength — making it a comprehensive frailty biomarker. Low scores (≤6) are associated with substantially elevated 5-year mortality, hospitalization risk, and fall incidence.
A systematic review and meta-analysis (Pavasini et al., 2016; n > 30,000) confirmed that each 1-point increment in SPPB score is associated with a statistically significant reduction in all-cause mortality risk. The same gradient is observed for hospital readmission, nursing home admission, and incident mobility disability.
From a frailty perspective, SPPB reflects the physical phenotype dimension of the Fried frailty criteria — slow gait speed and weak lower-limb strength — while the balance subtest adds information on postural control and fall risk not captured by gait alone.
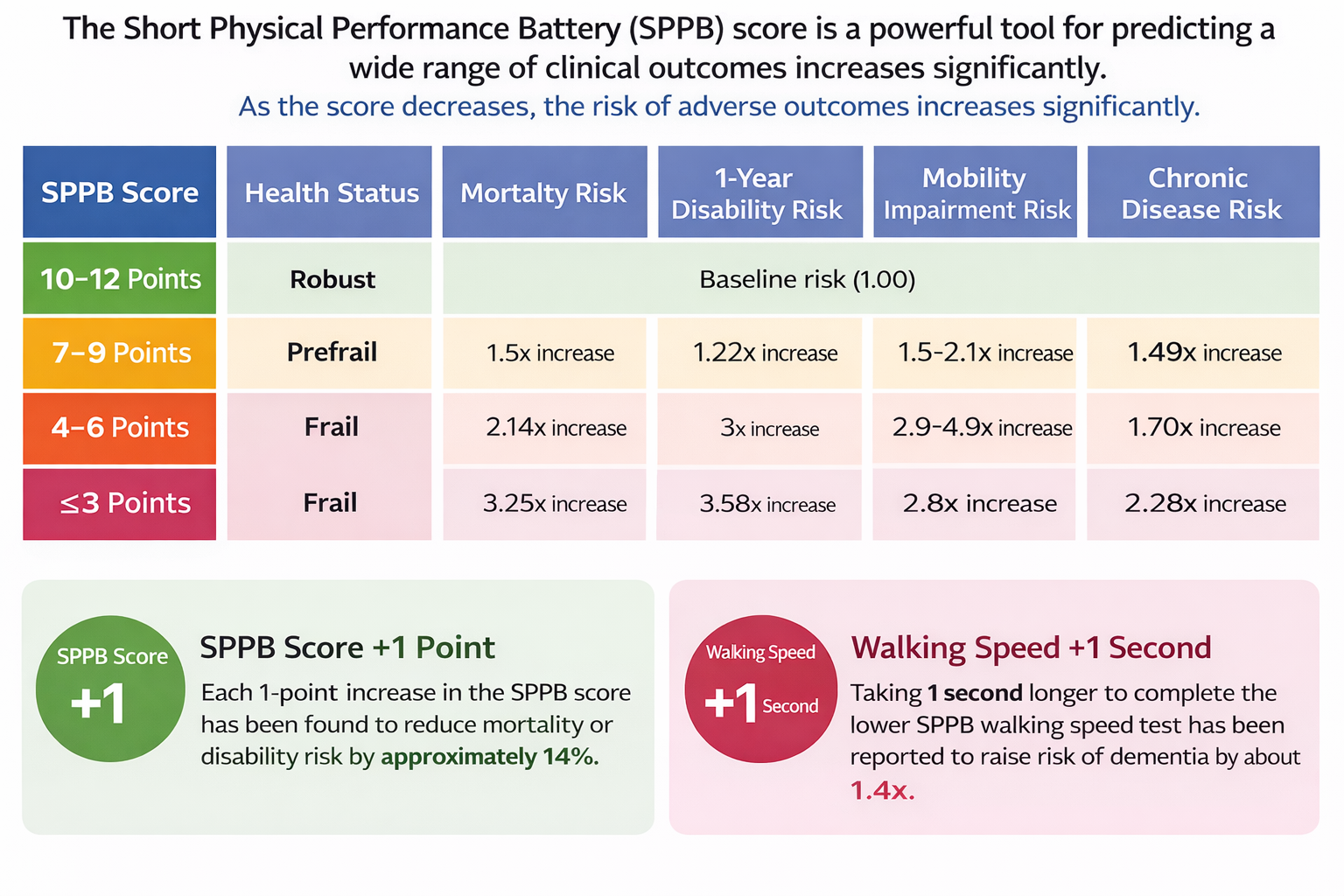
SPPB scores predict 5-year mortality, fall risk, and hospital admission. Each additional point corresponds to meaningfully reduced adverse outcome risk.